


by Michelle Garber (California, U.S.A.)

A Mean Girls-style graphic on a bright pink background reads “Burn Book (IBD version).” It has doodles scribbled over the text, including drawings of intestines and the poop emoji.
Inspired by Mean Girls and high school yearbooks, I created an “IBD Burn Book” to shed light on the invisibility of IBD and emphasize the importance of empathy when interacting with someone with IBD.

A yearbook-style photo collage of Michelle smiling and looking happy, with phrases like “don’t worry about me, how are you?” and “class superlative: biggest yes person.” In the background are the repeating words “smiling, outgoing, healthy, strong, energetic, reliable, lucky, blessed, positive, spontaneous, daughter, friend, sister, student, advocate, outspoken, happy.”
When you first open the Burn Book, you’ll see that my “Mask” has been crowned Prom Queen. The images on this page are from moments when I had my mask on—when I pretended to be “fine.” The background words reflect how others perceive me more positively when I wear this mask, which is why it was elected Prom Queen.
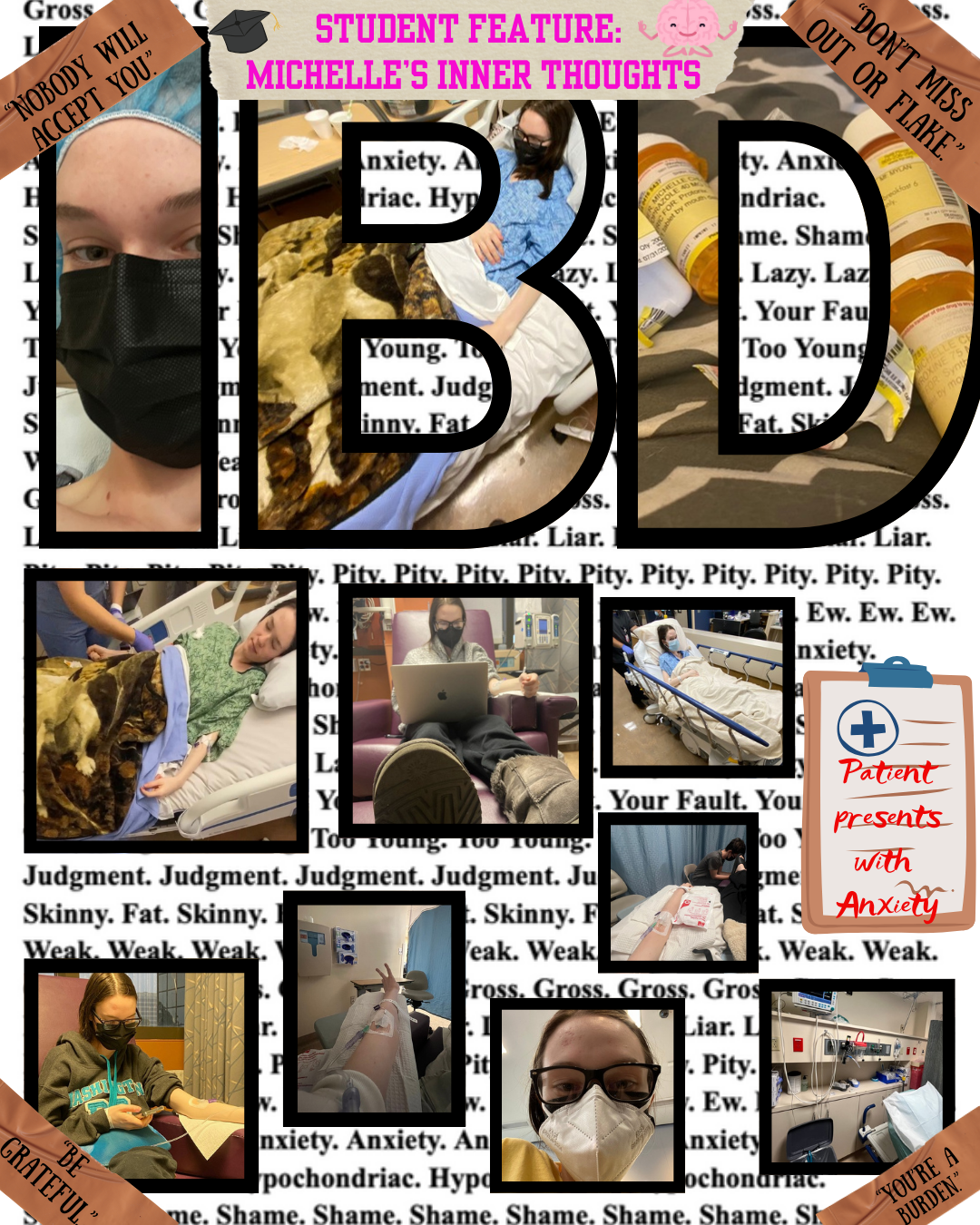
A yearbook-style photo collage of Michelle looking tired in various medical settings (the hospital, getting infusions) with phrases like “don’t miss out or flake,” “nobody will accept you” and “patient presents with anxiety.” In the background are the repeating words “gross, liar, pity, ew, anxiety, hypocondriac, shame, lazy, your fault, too young, judgement, skinny, fat, weak.”
The next page is a Student Feature of my Inner Thoughts. Here, I am without my mask. This contrast serves as a reminder that appearances can be deceiving—what you see on the outside isn’t always real; it might just be a mask.

Michelle’s ‘not hot’ list has a pink background with white squares. The following phrases are X’ed out in red pen: “I don’t want to touch you,” “so you’ve got bad genes?,” “i could never live like that,” “you’re too young to be sick,” “at least it’s not cancer,” “you look like a holocaust survivor,” “i have IBS too!,” “have you tried yoga?,” “gross,” “It’s all the junk food you’re eating,” “look on the bright side, you lose weight easily,'“ and “i guess this means we’ll have to adopt.”
Following that is a Not Hot List, which consists of a collection of phrases people should never say to someone with IBD. (Sadly, every one of these remarks has been said to me).
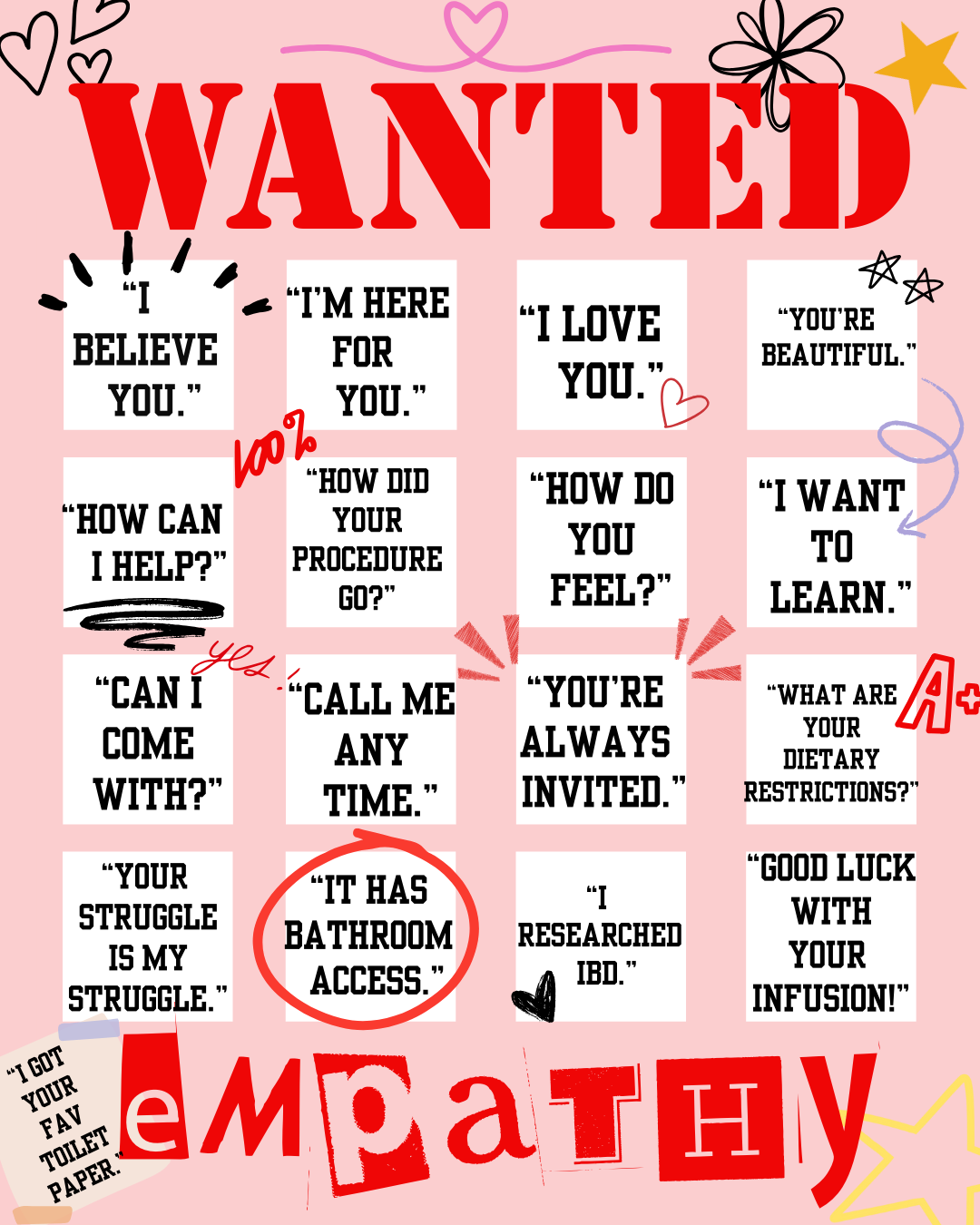
A pink poster labeled “wanted: empathy.” In each square, there is a different phrase: “I believe you,” “I’m here for you,” “I love you,” “you’re beautiful,” “how can I help?,'“ “how did your procedure go?,” “how do you feel?,” “I want to learn,” “can I come with?,” “call me any time,” “you’re always invited,” “what are your dietary restrictions?,” “your struggle is my struggle,” “it has bathroom access,” “I researched IBD,” and “good luck with your infusion!.” The phrases are emphasized with stars, hearts, and stickers that read “100%!” “yes!” and “A+.”
The final page of the Burn Book is a WANTED poster—for empathy. Instead of harmful comments, this page lists empathetic phrases one should say to someone with IBD. Essentially, it serves as the “Hot List” in Mean Girls or high school terminology.
———
Invisible illnesses come with their own set of challenges—such as a widespread lack of awareness—but the focus here is how easily someone with IBD can hide their struggles. Smiling through the pain, pretending to feel well—it becomes second nature. I’m not the first person to wear a “mask” to feel accepted or to make others comfortable, and I certainly won’t be the last.
The reality, though, is that IBD is a constant battle. Even if you see me dancing with friends, traveling, or enjoying a big meal, I am still struggling. The takeaway? You never truly know what someone else is going through, so always choose kindness. More importantly, choose empathy. If you do know what someone is going through (specifically IBD in this case), be especially mindful of your words and actions. While you might assume your words and actions don’t affect us, remember—we’ve had a lot of practice hiding our pain.















{kind=link}