Newly diagnosed with IBD? I wish you knew these first.
Growing up as a teenager, I was a perfectly healthy child. I ate regularly; I was active and a bright kid who never had any particular routine or lifestyle that I used to follow. But everything started turning upside down once I started seeing symptoms. An bigger tragedy was when I almost felt like the game had ended after being diagnosed. No! Not at all. The actual game starts only after the diagnosis. Our bodies are always changing with IBD. From one day to the next, we don’t know how we are going to feel or what is going to happen. So it is of the upmost importance to know yourself and your body first. Ignorance certainly isn’t bliss here. If you feel like IBD is ruling your life, it’s time to take back the control. Here are the 10 things which I would like to share with all those who are newly diagnosed with IBD:
Educate yourself: Knowledge is power. Understanding IBD leaves you better equipped and empowered to manage it. There are many patients out there without enough knowledge about their IBD. It’s our responsibility to know everything we can about our disease and also our bodies. Take the time to learn everything you can. Read and discuss as much as possible with your doctors.
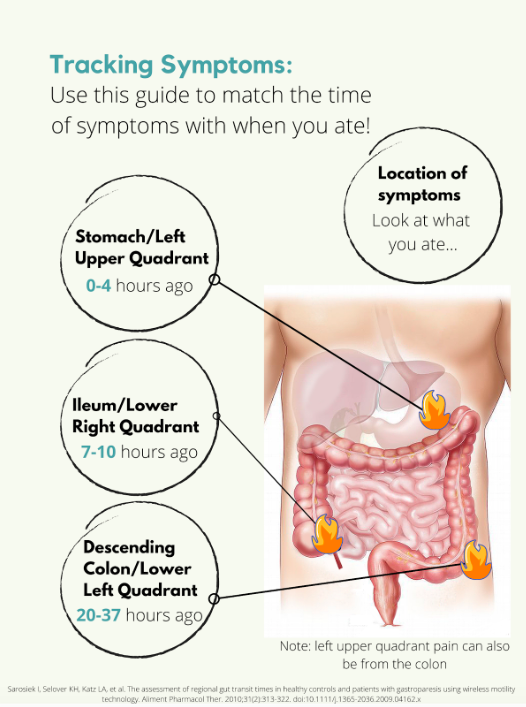
Track your symptoms and triggers: Learn about your own symptoms and triggers. Many doctors suggest maintaining a food diary so that your doctor may be able to use the data you gathered to help guide your treatment plan. We can understand our daily life and limit what happens to us by doing this.
Never miss your regular follow ups: After reaching my first remission, I assumed I was completely cured and had stopped my regular check-ups and follow ups with my doctor. The penalty for being so ignorant came with a cost of having the next severe flare up within the next few months which completely drained me and pulled me back to square one. IBD is a disease which needs to be managed and if you feel symptom free, you are not cured, it’s just that your medicines are working and controlling your symptoms. So it is important to have regular consultations with your doctor and monitor the functioning of your systems.
Make every appointment count: Be well prepared as to what you need to discuss with your doctor before hand as most of the appointments will be limited to 10-15 minutes and you tend to lose out on discussing important stuff. You can even jot down pointers on paper before entering the doctor's cabin.
Don't be afraid to ask for more information: The time slot allotted for each appointment may be limited. That doesn't mean you need to limit your queries and clarifications. Make the best of that limited time. For instance, if you’re being treated with steroids, ask for detailed information about how this medication could influence how you feel, the side effects, mood swings, weight gain, and such.
Know your treatment: First, know what kind of treatment the doctor has put you on. Whether it is the traditional treatment or biologics or allopathy or any other alternative therapies. Understanding your treatment can help you know what is happening to your body and analyse your recovery rate to attain symptom free life by choosing the best that suits your body as what suits others may not you and vice versa.
Emotional health is equally important as your physical health: There could be days when your entire body hurts and there is nothing you can do. There could even be days when you don’t even want to move because you are so exhausted. During those days it’s not easy to control your emotions as you tend to feel more low and helpless. But you can still fight back by choosing to feel “it's OK”. Don’t let your IBD control you.
Coping with Stress: Stress doesn’t cause IBD, but it can sometimes make symptoms worse. Stress relief is crucial if stress provokes your flare-ups. Learning how to cope with stress and anxiety isn’t always easy. But it’s really important for us to keep stress under control. Yoga, meditation and music could be a few tools that may be helpful in this.
Reach out for help when needed: IBD can be an embarrassing disease. It’s normal to feel alone sometimes. At a young age, we are taught not to discuss what happens behind a bathroom door. This can leave those of us with IBD, feeling extremely isolated and even hopeless. This can impact our self-esteem and quality of life. It's utmost important to have some go to people who understand these challenges and support us in every step of our journey.
Nutrition matters: Understand how your system works and choose what goes into it rightly. When the intestine is under attack, it has a hard time absorbing nutrients. Therefore it's important for us to be aware of what we eat. Follow a low residue diet to relieve abdominal pain and diarrhea. If you have strictures, it is especially important to avoid nuts, seeds, beans and kernels.
These are few of the things which I feel we need to keep in mind and plan our lifestyle when newly diagnosed. Knowing these pointers at the initial stages makes our lives much easier.